
 Locations
LocationsIs being middle income a precondition? The “syndemic” of chronic disease, social inequality, and COVID-19 in LAC
November 11, 2020

As COVID-19 has spread across the globe, it has become increasingly clear that the virus’s health impacts are being shaped by larger social, economic, environmental, and political factors. In this vein, Dr. Richard Horton (editor-in-chief of leading medical journal The Lancet) recently argued that we should in fact not think of COVID-19 as a pandemic—but rather, as a “syndemic.”
The concept of a “syndemic” goes beyond a purely biological conceptualization of disease to also consider the broader social context in which it interacts. As described by Singer et al (2017), “syndemics involve the adverse interaction between diseases and health conditions of all types (eg, infections, chronic non-communicable diseases, mental health problems, behavioral conditions, toxic exposure, and malnutrition) and are most likely to emerge under conditions of health inequality caused by poverty, stigmatization, stress, or structural violence.”
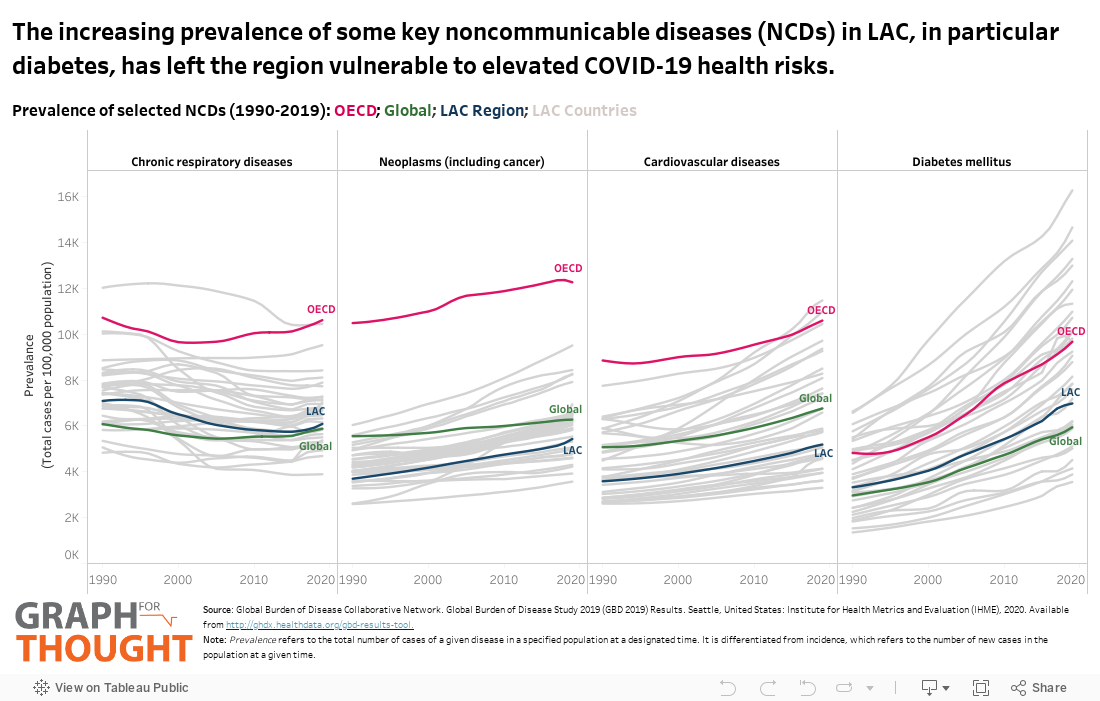
In the context of COVID-19, this is particularly important as underlying health conditions have been found to be associated with worse COVID-19 health outcomes (i.e. higher risk of hospitalization, ICU admission, or death). While it is still too early to know the full extent to which different health conditions interact with COVID-19 in different contexts, it is broadly agreed that key non-communicable diseases (NCDs) (such as diabetes, cardiovascular disease, respiratory disease, and cancer) and key risk factors associated with them (such as obesity, smoking, alcohol use, physical inactivity, and pollution) are of particular concern. Indeed, the recently released Global Burden of Disease Study finds that “the interaction of COVID-19 with the continued global rise in chronic illness and related risk factors…over the past 30 years has created a perfect storm, fueling COVID-19 deaths.” Using data from this study, this #GraphForThought zooms into the LAC region to see how key NCDs and NCD risk factors have been changing in recent decades—setting the stage for potentially elevated COVID-19 risk.
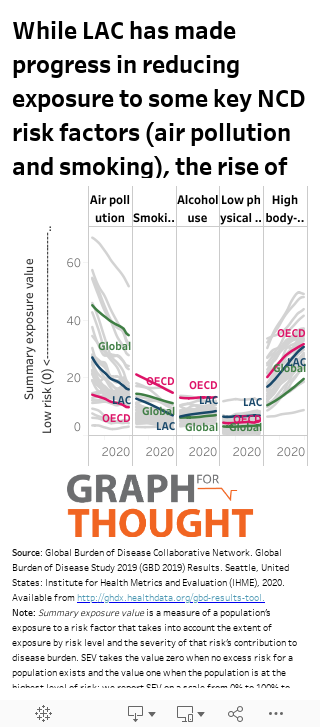
The graphs show how the prevalence of NCDs (measured as total cases per 100,000 population) and the exposure to NCD risk factors (measured by a summary exposure value ranging from 1-100) have changed over the period 1990-2019. We can see how trends in the LAC region (dark blue) compare with global trends (green) and OECD trends (pink); as well as the unique trends for individual LAC countries (grey). Note that you can see which country each line refers to by hovering your cursor over the datapoint.
It is first important to note the wide heterogeneity across the region—as shown by the dispersion of the grey lines. While the general direction of trends is similar across LAC countries (increasing or decreasing), the levels are vastly different—particularly in the case of diabetes, air pollution and obesity. If we look at the direction of trends over time, we see general increasing prevalence of NCDs (expect for chronic respiratory diseases) and we see mixed changes in exposure to risk factors (decreasing exposure to air pollution and smoking; minimal change in low physical activity; and increasing exposure to alcohol use and obesity). Trends in LAC tend to parallel global and OECD trends; and LAC tends to outperform OECD countries. However, in comparison to the global aggregate – LAC performs worse in terms of diabetes, obesity, low physical activity, and alcohol use. In particular, the rapid rise in diabetes and obesity in the LAC region is concerning—with extremely elevated levels in several countries (largely within the Caribbean).
This rise of obesity and diabetes is often associated with countries’ transition to middle income status—as rising economic growth, increasing globalization and rapid urbanization foster changes in people’s diets and lifestyles. These aggregate trends, however, also might be hiding a second story of shifting burden of disease within LAC countries. As a recent study on changing patterns of obesity in region by Jiwani et al (2019) acknowledges—"although obesity has long been considered a condition of the elite and a mark of wealth, published literature in the past decade suggests that it can no longer be attributed to higher socioeconomic status.” Using data for 13 LAC countries, the authors find that while the prevalence of obesity is increasing in the region overall, the “largest increases have been among rural residents and the most disadvantaged groups.” The interaction of inequality and NCDs is particularly concerning in a region such as LAC, which is marked by some of the highest levels of inequality in the world.
Marginalized communities face unique constraints to achieving better health outcomes such as limited access to healthy diets, higher stress from financial burdens or situations of violence, limited access to healthcare, or limited access to safe areas to exercise. In the context of COVID-19 this raises concern for greater adverse health impacts in already marginalized communities—as these are also same communities that are less likely to be able to stay at home given the need continue working (often in jobs that are unable to be performed remotely), and more likely to be living in housing conditions that have limited access to sanitation for handwashing or rooms too small for social distancing.
Thus the capacity to tackle COVID-19 is not just a question of a country’s health sector capacity, but also a function of the population’s underlying health vulnerabilities. In this way, finding solutions to COVID-19 in LAC will require going beyond medical interventions to also address the structural social disparities that have made certain populations more vulnerable in the first place. It is indeed a question of governance. As Dr. Horton notes, “the pursuit of a purely biomedical solution to COVID-19 will fail. Unless governments devise policies and programmes to reverse profound disparities, our societies will never be truly COVID-19 secure… Approaching COVID-19 as a syndemic will invite a larger vision, one encompassing education, employment, housing, food, and environment.”